Toll FREE: 1.877.965.2140
International: 1.805.322.0005


Cholesterol Metabolizer®
As low as $19.95 per bottle
What is Cholesterol?
Cholesterol is an organic lipid molecule, (a sterol) which is biosynthesized by all animal cells. It is an essential structural component of all animal cell membranes and is essential to maintain both membrane structural integrity and fluidity. Cholesterol allows animal cells to function without a cell wall.
With all the bad press these days about cholesterol, many people may be surprised to learn that cholesterol is actually an essential part of every cell's structure. It is needed for proper brain and nerve function and is the basis for the manufacture of sex hormones as well.
To understand this apparent contradiction as to how cholesterol can be both "bad" and "good", it is important to understand that cholesterol is manufactured in the liver and transported through the bloodstream to the sites where it is needed. Since It is a fatty substance; and because blood is mainly water; it has to latch on to molecules called lipoproteins in order to travel around successfully.
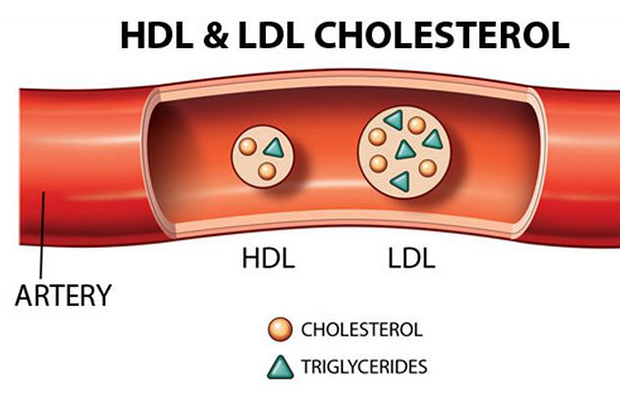
When we talk about "good" and "bad" cholesterol, we are actually distinguishing between the two different types of lipoproteins cholesterol latches on to:
1. high density lipoproteins (HDL's) are considered "good cholesterol" because they carry unneeded cholesterol away from the cells and back to the liver, where it is broken down for removal from the body. If everything is functioning as it should, this system remains in balance. However, if there is too much cholesterol for the HDLs to pick up promptly, or if there are not enough HDLs to do the job, cholesterol can form plaque that sticks to artery walls and may eventually cause heart disease.
2. low density lipoproteins (LDL's) are the major transporters of cholesterol in the bloodstream and are considered "bad cholesterol" because they carry fats out of the liver to the blood vessels. LDLs seem to encourage the deposit of cholesterol in the arteries.
Why are Serum Cholesterol Levels Important?
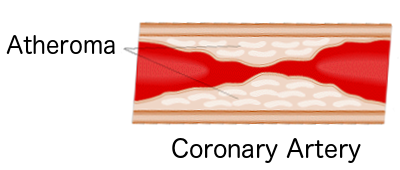
Heart disease is the leading killer of both men and women after the age of 45. High cholesterol is responsible for 70% of heart disease. It leads to arterial blockage, heart attacks, hardening of the arteries, blood clots, clogged arteries, and stroke. Over 26 million Americans have high cholesterol. High cholesterol it is not just a disease which effects adults. More and more it is being discovered that our teenagers and even preteens are walking around with this potentially life threatening condition!
It is also important to distinguish between serum cholesterol and dietary cholesterol. Serum cholesterol is the cholesterol in the bloodstream. Dietary cholesterol is cholesterol that is present in food. While eating foods high in dietary cholesterol can raise serum cholesterol, it is not the only source of serum cholesterol. Indeed, you would have some amount of serum cholesterol even if you never ate any food containing dietary cholesterol because the body produces its own cholesterol.
 The National Cholesterol Education Program has set the "safe" level of total serum cholesterol (including both LDL and HDL) at 200 milligrams per deciliter of blood 9mg/dl). A reading above 200 indicates an increased potential for developing heart disease. A level of 200 to 239 is borderline, and levels over 240 are considered to indicate high risk. The normal HDL level for adult men in the United States is 45 to 50 mg/dl, and that for women is 50 to 60 mg/dl.
The National Cholesterol Education Program has set the "safe" level of total serum cholesterol (including both LDL and HDL) at 200 milligrams per deciliter of blood 9mg/dl). A reading above 200 indicates an increased potential for developing heart disease. A level of 200 to 239 is borderline, and levels over 240 are considered to indicate high risk. The normal HDL level for adult men in the United States is 45 to 50 mg/dl, and that for women is 50 to 60 mg/dl.
It is suggested that higher HDL levels, such as 70 or 80 mg/dl, may protect against heart disease. An HDL level under 35 mg/dl is considered risky. So if you have a cholesterol reading of 200, with HDL at 80 and LDL at 120, you are considered at low risk for heart disease. On the other hand, even if you have a total cholesterol level well under 200, if your HDL level is under 35, you would still be considered at increased risk of developing cardiovascular disease. In other words, as your HDL decreases, your potential for heart problems intensifies, even if your total is on the low side.
Risk Factors for High Cholesterol
High cholesterol is responsible for 70% of heart disease and is the leading killer of both men and women after the age of 45. It leads to arterial blockage, heart attacks, hardening of the arteries, blood clots, clogged arteries, and stroke. There are a number of factors that influence a person's cholesterol levels. They include diet, age, weight, gender, genetics, diseases and lifestyle.
- Diet
- Age
- Weight
- Gender
- Genetics
- Disease
- Lifestyle
Most of us consume foods high in dietary fat. Foods which are fried or are high in animal fats will directly raise blood serum levels of "bad cholesterol"
Foods which are high in simple carbohydrates such as sugars, bread, pasta and sweets indirectly raise "bad cholesterol" levels as they are converted into "bad cholesterol" by the liver. This explains why some vegetarians have high cholesterol.
The blood levels of cholesterol tend to increase as we age--a factor doctors consider when deciding treatment options for patients with certain cholesterol levels.
People who are overweight are more likely to have high blood cholesterol levels. They also tend to have lower HDL levels. The location of the excess weight also seems to play a role in cholesterol levels. A greater risk of increased cholesterol levels occurs when that extra weight is centered in the abdominal region, as opposed to the legs or buttocks.
Men tend to have higher LDL levels and lower HDL levels than do women, especially before age 50. After age 50, when women are in their post-menopausal years, decreasing amounts of estrogen are thought to cause the LDL level to rise.
Some people are genetically predisposed to having high levels of cholesterol. A variety of minor genetic defects can lead to excessive production of LDLs or a decreased capacity for their removal. This tendency towards high cholesterol levels is often passed on from parents to their children. If your parents have high cholesterol, you need to be tested to see if your cholesterol levels are also elevated.
Diseases such as diabetes can lower HDL levels, increase triglycerides and accelerate the development of atherosclerosis. High blood pressure, or hypertension, can also hasten the development of atherosclerosis, and some medications used to treat it can increase LDL and triglycerides and decrease HDL levels.
Factors that negatively affect cholesterol levels also include high levels of stress, which can raise total cholesterol levels, and cigarette smoking, which can lower a person's HDL level as much as 15 percent. On the other hand, strenuous exercise can increase HDL levels and decrease LDL levels. Exercise also can help reduce body weight, which, in turn, can help reduce cholesterol. Recent research has shown that moderate alcohol use (one drink per day for women, two drinks a day for men) can raise HDL cholesterol and therefore reduce the risk of heart attack. Despite such research, it is difficult to recommend the habitual use of alcohol because there are also negative health consequences associated with alcohol use and a high potential for abuse
Statin Drugs are Dangerous
If your doctor has prescribed Lipitor, Zocar, Provacol or other Statin Drugs, you owe it to yourself to read the warnings that accompany this medicine. Read them carefully. The print is small but take your time and learn about the dangers you are facing with these dangerous drugs. You are probably killing yourself while at the same time feeling drowsy, dizzy, depressed, and lacking in energy and your usual vitality. That's because these dangerous toxins are slowly poisoning you and increasing your risk of cancer, heart disease, depression, suicide, and general lack of interest in life.
If you're taking a statin drug don't wait for your doctor to warn you of the substantial risks. Consider this fact: in the last 25 years (roughly the time that statins have been on the market), the incidence of congestive heart failure has tripled.
Furthermore, many patients who take statin drugs suffer with sleep disturbances, memory loss, sexual dysfunction, depression and a rare lung disease that can kill if left untreated.
A visit to any of the numerous health-oriented forums on the internet will quickly reveal hundreds of posts from dissatisfied statin users, describing an alarming array of side-effects: the most common being extreme fatigue, nausea, gastrointestinal problems, and muscle weakness and pain. Complaints about doctors' inability to link their recent health problems with statin use are frequent. In many instances, users report that they put two-and-two together themselves, stopped taking the drugs, and experienced significant or even complete remission of their symptoms.
Frequent side effects are no doubt a major reason why up to 75% of people taking statins discontinue their use.
Of course, defenders of statins are quick to point out the low incidence of adverse effects in controlled, randomized clinical trials as proof of their alleged safety. If you look at these studies closely however you will find that when recruiting for statin clinical trials, researchers carefully screen for, and exclude, a wide range of individuals including women of childbearing age, those with a history of drug or alcohol abuse, poor mental function, heart failure, arrhythmia, and other cardiac conditions, liver and kidney disorders, cancer, "other serious diseases", and "hypersensitivity" to statins. Thus, the disparity between the widespread "real-world" prevalence of side effects from statin use and the low prevalence of side effects in clinical trials is hardly surprising. These trials exclude groups that comprise a significant proportion of the real world population, and can hardly be taken as a realistic barometer for the expected incidence of side effects in the general population.
And even with these strict exclusion criteria, there is evidence to show that the clinical experience with statins has been far from trouble-free. Data for the largest statin trial, the Heart Protection Study (HPS), suggest that the daily 40mg dose of simvastatin used was nowhere near as well tolerated as the authors would have us believe. A substantial number of patients did not enter the trial after a six week run-in before randomization; of the 63,603 potential trial participants who entered the original screening, only 32,145 proceeded to the run-in phase. Of these, 11,609 patients - over one third - dropped out before the official start of the trial.
Regardless of what Statin manufacturing companies would have us believe, the dangers from statin use are very real, as illustrated by the tragic death of Mrs. Elnoisa Calabio. Mrs. Calabio's story was presented at an FDA public hearing in May 2000:
"On October 7, 1999, at the age of 48, registered nurse, wife and mother, Elnoisa Calabio, succumbed to the end stages of irreversible dermatomyositis and interstitial pulmonary fibrosis directly caused by her use of a prescribed cholesterol-lowering medication, simvastatin (Zocor). Mrs. Calabio had no substantial risk factors for heart disease. Her blood pressure was controlled. Her cholesterol was slightly high, but not considered dangerous. Tragically, in her last days she knew that the cholesterol lowering drug her doctor had recommended to extend her life was in fact the cause of her fatal illness."
Sadly, Mrs Calabio's family is hardly alone in grieving the needless, statin-induced loss of a loved one. In August 2001, pharmaceutical giant Bayer was forced to withdraw Baycol (cerivastatin) from the market, after at least fifty-two deaths had been linked to the drug. Baycol was causing rhabdomyolysis, a condition characterized by severe muscle damage. This rare disorder occurs when a large number of skeletal muscle cells die, subsequently releasing massive amounts of muscle protein into the bloodstream. This muscle protein saturates the kidneys, effectively overwhelming their filtration capacities. Indeed, kidney failure was reportedly a major cause of death amongst the Baycol victims. Baycol is not unique in its ability to damage muscle - all the statins have been shown to produce muscle disorders in susceptible patients, and muscle pain is one of the most common reasons for patients being taken off statin drugs.(33) Researchers recently reported that some patients may suffer muscle deterioration caused by statins while still maintaining normal levels of creatine kinase, the most commonly used indicator of muscle damage.
Statin Drugs Can Cause Liver Damage
Statin drugs can cause abnormalities in liver function, occasionally causing mild hepatitis. In fact people with liver problems can not take Statin drugs at all even if they have very high LDL levels. Between one to three percent of people who start taking statins will have a mild to severe elevation in their liver enzymes. Thus, for about one in 5,000 patients, liver enzymes need to be monitored periodically to make sure the liver still functions reasonably.
Most physicians do blood tests when they start treating people with drugs like Lipitor. They are looking for elevated liver enzymes released into the blood. These enzyme levels are always present, but increase if there is damage to liver cells. All of the statins can cause an increase in these markers in the blood, and cause damage to the liver (hepatotoxicity). It appears that the likelihood of this happening is related to the dose of statins used. The higher the dose, the more likely it is that we will see increases in these markers. Increases in these markers. have been observed in 2-5 percent of patients taking statin drugs. Usually, the increase is reversed after the drug is stopped with no permanent liver damage. But If the drug is not stopped, there can be permanent liver damage.
Because statins have been linked to liver problems and muscle weakness. Many researchers have concluded that patients at low risk of heart disease should very carefully weight the benefits of using statins against the potential risks.
Statin Drugs Can Cause Nerve Damage
Shortly after statin drugs reached the global market, a Danish physician noticed reports of nerve damage in 14 patients. In 1999, he and his colleagues reported on seven of those cases, then wondered how commonly the side effect, called polyneuropathy, occurs.
For this study, the researchers probed medical records of all 460,000 residents of a Danish county. They excluded patients with diabetes, which can cause nerve damage, and they accounted for the effects of any other medicines with neurological side effects.
The new study, reported in May in the journal Neurology but largely overlooked by heart experts, comes as drug manufacturers are working on next-generation cholesterol treatments — and as more baby boomers are urged to take the medications to lower their risk of heart attacks and strokes.
Study co-author David Gaist of the University of Southern Denmark says the findings ought to alert doctors to the possibility of nerve damage among patients on statins but should not discourage their use.
Other experts agree. Sidney Smith, chief science officer for the American Heart Association, called Gaist's study interesting, but pointed out that studies of the drugs' effectiveness in 50,000 people have not shown nerve damage as a significant finding. "Nevertheless, physicians should be aware of symptoms that might be related," he says.
Statin Drugs Can Cause Muscle Damage
According to Dr. Paul S. Phillips, a cardiologist at Scripps Mercy Hospital in San Diego, California, satin drugs are not only very expensive but have many side effects and are potentially very dangerous.
Phillips has studied patients in his practice and has concluded that all statins have the potential to cause muscle damage (myopathy), which can lead to a fatal condition called rhabdomyolysis, in which the muscle completely breaks down. Bayer's statin drug Baycol was taken off the US market in August 2001, after the Food and Drug Administration (FDA) received at least 52 reports that people taking Baycol had died of rhabdomyolysis. Another 50 have since died, Phillips said.
He said many of his patients complain of severe muscle aches and fatigue while taking statins, even though they show no signs of muscle damage when their blood is tested for a key enzyme called creatine kinase. High levels indicate trouble. The American Heart Association ( news - web sites) and the American College of Cardiology have recommended that patients be taken off statins if their creatine kinase levels are 10 times normal.
Phillips decided to further study his patients with normal creatine kinase levels. He took samples of their muscle tissue while they were taking statins and also during an 8-week period when they were taken off the drugs. In a paper in the October 1st issue of the Annals of Internal Medicine, he reported that of the first four people studied, all had muscle tissue abnormalities that are rarely seen. These four patients also were very weak in stair-stepping and hip adductor strength tests. When the patients went off statins, they felt better, they were stronger and their tissue samples looked normal again, Phillips said. He is testing more patients and gathering more data, but said he thinks that the currently recommended muscle enzyme test may not detect muscle damage in some people who take statins.
Statin drugs deplete essential CoQ10 reserves in the body
Coenzyme Q10 -- also called ubiquinone, which means "occurring everywhere" -- plays an important role in the manufacture of ATP, the fuel that runs cellular processes. In addition to this fundamental role in energy production, CoQ10 acts as a potent antioxidant. Though it is present in every cell in your body, it is especially concentrated in the very active cells of your heart. Not surprisingly, CoQ10 is extremely important for cardiovascular health, with high levels being found in healthy heart tissue.
Statins have been shown to deplete the body of Coenzyme Q10. Statins block enzyme pathways involved in the production of cholesterol, thereby lowering cholesterol levels. But the same enzymes that are involved in the production of cholesterol are also required for the production of coenzyme Q10; not surprisingly, lower cholesterol levels in statin users are accompanied by reduced levels of CoQ10.
Depriving the heart of CoQ10 is like removing a spark plug from your engine -- it just won't work. Low levels of CoQ10 are implicated in virtually all cardiovascular diseases, including angina, hypertension, cardiomyopathy and congestive heart failure.
Ironically, while statins are taken to reduce the risk of atherosclerotic heart disease, their CoQ10-robbing effects have been linked to an increased risk of congestive heart failure. Figures from the National Center for Health Statistics show that since the early nineties - when statin drugs began hitting pharmacy shelves - the incidence of congestive heart failure has risen sharply.(37) CHF, in fact, is the fastest growing cardiovascular disorder in the United States. Sadly, there is no cure for CHF short of a heart transplant. Peter H. Langsjoen, MD, a foremost authority on the use of coenzyme Q10 in the treatment of heart disease, has little doubt as to the culprit behind this sharp rise in CHF:
"In my practice of 17 years in Tyler, Texas, I have seen a frightening increase in heart failure secondary to statin usage, "statin cardiomyopathy". Over the past five years, statins have become more potent, are being prescribed in higher doses, and are being used with reckless abandon in the elderly and in patients with "normal" cholesterol levels. We are in the midst of a CHF epidemic in the US with a dramatic increase over the past decade. Are we causing this epidemic through our zealous use of statins? In large part I think the answer is yes."
While CoQ10 is not only critically important for healthy cardiovascular function; the brain is also highly vulnerable to CoQ10 deficiencies. When healthy young men were given either statin drugs or a placebo, those taking lovastatin displayed significant deterioration in cognitive function after only three weeks of treatment.(37) Brian Vonk, M.D., of The Optimal Wellness Center, reported recently that, in his own experience and that of his colleagues:
"statins cause depression or loss of motivation in the majority of patients, probably due to alteration of cholesterol metabolism in the brain. As a result, many of these patients are also on [antidepressant] drugs (e.g. Zoloft, Paxil, Prozac)."
Since the introduction of Statin drugs in 1987, Merck has known that statins deplete CoQ10 reserves, and knew that this could contribute to heart disease. In 1990, Merck sought and received a patent for Mevacor and other statin drugs formulated with up to 1,000 mg of coenzyme Q10 to prevent or alleviate cardiomyopathy, a serious condition that can cause congestive heart failure. Merck however, has not brought these combination products to market, nor have they educated physicians on the importance of supplementing CoQ10 to offset the dangers of these drugs to the heart. Because they hold the patent, other drug companies are prevented from coming out with a statin/CoQ10 product.
Statin drugs and Cancer
In 1996 the Journal of the American Medical Association published an extensive review of the research studying the link between cholesterol-lowering drugs and cancer. The authors, Dr Thomas Newman and Dr. Stephen Hulley, stated: "All members of the two most popular classes of lipid-lowering drugs (the fibrates and the statins) cause cancer in rodents, in some cases at levels of animal exposure close to those prescribed to humans." In light of their findings, the authors recommended that: "lipid-lowering drug treatment, especially with the fibrates and statins, should be avoided except in patients at high short-term risk of coronary heart disease."
Newman and Hulley's recommendation has been all but ignored. Statins are being recommended and prescribed, not just to people at high short-term risk, but to perfectly healthy people who show no clinical manifestations of CHD whatsoever, except for the non-disease of hypercholesterolemia. Even children with "elevated" cholesterol levels are being urged to commence statin therapy
Drug companies and health authorities repeatedly assure us that statins are wonderful low-risk drugs that are well tolerated in most people. They claim that clinical trials have shown no increase in cancer incidence with statin use, but the longest of these studies ran for only 6 years (excepting the EXCEL trial, which showed an increase in total mortality after 1 year of lovastatin use, and for which no subsequent mortality data has ever been released(44)). Cancer is a chronic disease that may take decades to manifest itself as a life-threatening illness - can we really conclude from trials lasting five to six years that statins are safe for lifetime use? Even heavy smokers are highly unlikely to develop cancer within six years of taking their first puff; most continue for decades before they come to realize the true value of those little warnings adorning cigarette packets.
Because rodent studies routinely use far higher dosages of drugs than those prescribed to humans, some have questioned the relevance of Newman and Hulley's findings. In many studies, rodents have been shown to eliminate drugs much faster than humans, necessitating higher dosages to maintain constant blood levels of the drug. The authors noted, however, that when the drug exposure was considered in terms of blood levels, carcinogenicity occurred at levels close to those seen in humans. In the same journal in which this review appeared, a commentary critical of Hulley and Newman claimed that higher dosages used in rodents placed inordinate stress on their gastrointestinal tracts, and that most of the cancers seen in rodent studies were malignancies of the gastrointestinal tract and liver.(45) Given that gastrointestinal distress and liver toxicity are among the most frequently reported side effects in patients prescribed statins, this proffered explanation provides little reassurance.
The claim that statin trials have not shown any increase in cancer is disputed by the recent PROSPER trial, which found a 25% increase in newly diagnosed cancers among elderly individuals treated with pravastatin. While there were 20 less deaths from CHD and stroke in the treatment group, 24 more deaths from cancer were observed, and, in an ominous confirmation of animal findings, one of the highest increases was observed for gastrointestinal cancers.(46) The PROSPER authors dismissed these findings by referring to a pooled analysis they performed of eight statin trials that lasted three or more years, which showed no statistically significant difference in cancer incidence between the placebo and statin groups (6.9% versus 7.1%, respectively). However, most of these trials involved younger subjects. Because cancer risk increases with age, such a comparison bears little relevance to the PROSPER results. Due to their heightened risk, elderly subjects may act as a far more sensitive barometer to any cancer-promoting capacity possessed by statins.
Furthermore, as researcher Uffe Ravnskov, M.D., PhD., recently pointed out, the PROSPER researchers' analysis did not include skin cancer.(47) Considering the relatively short-term nature of statin trials, it is the incidence of such an easily detectable, superficial cancer that would provide the strongest clue as to the future cancer-causing potential of statins. Only two of the statin trials have reported skin cancer incidence; the 4S and HPS simvastatin trials. Increases in skin cancer were noted in both.
In the CARE trial, breast cancer, another readily detectable malignancy, developed in 12 women from the treatment group but in only one of the control individuals - a highly significant difference.(50) Breast cancer was also the malignancy for which the greatest increase was noted in the PROSPER trial. The possibility that statins will lead to future increases in cancer incidence cannot be flippantly dismissed.
To maintain their lipid-lowering effects, statins must be administered on a life-long basis. The reports of carcinogenicity from rodent studies and increases in superficial cancers noted in human trials warrant extreme caution. Given the complete lack of data on the effects of decades of statin administration, users can consider themselves part of a mass experiment in progress, the outcome of which is largely unknown.
Warnings for statin use to be limited to high-risk patients - where dramatically shortened life expectancies may override any concerns about long-term side-effects -have been completely overshadowed by the relentless promotional efforts of drug companies and enthusiastic endorsements from health authorities who are besides themselves at finally having clinical data that, on the surface, appears to support the lipid hypothesis.
Are we witnessing the unfolding of another officially-endorsed health disaster? Only time will tell. For those who do not want to find out the hard way, there are numerous non-drug measures that can help alleviate the risk of CHD. Randomized trials involving increases in fish/fish oil and/or fruit and vegetable consumption have produced risk reductions in mortality similar, and in some instances superior, to those seen in statin trials;(51-57) these safe, natural food items, as well as exercise, stress reduction, sound sleep, and a low glycemic load diet (i.e.., a low-to-moderate carbohydrate diet comprised of unrefined low glycemic foods), would be a far more judicious preventive alternative for those with no clinical signs of CHD.
How to Support Healthy Cholesterol
There are several components to a program to support healthy cholesterol:
1. The single most important thing a person can do is to eat a healthy diet. Specifically, eliminate and/or cut back on fried foods, fatty foods and foods rich in simple carbohydrates. Unfortunately, changing lifelong eating habits can be very difficult and so many people just won't do it.
2. Exercise is an excellent method for improving circulation and cardiovascular function in general. You can support healthy cholesterol levels and healthy blood pressure with no change in diet just by walking a half hour a day. Furthermore, because exercise is very effective in reducing stress and because hormones (released during stress) stimulate the liver to produce "bad cholesterol", exercise helps support healthy cholesterol levels through its stress-reducing action.
3. Support healthy cholesterol through the use of the following endogenous (occurring naturally in the body) dietary supplements: Beta Sitosterol, Beta Glucan, Soy Isoflavones & Chromium Picolinate. Though some exogenous (NOT occurring naturally in the body) supplements such as Guggu and Policosanol may be supportive as well, exogenous supplements in general will only support healthy cholesterol for about six months. Beyond that you will NOT get any additional support from continuing to take them.
Support Healthy Cholesterol levels with 100% Natural Cholesterol Metabolizer®
- Cholesterol Metabolizer® is a unique, 100% natural, cholesterol support formula which is guaranteed to support healthy cholesterol levels.
- Cholesterol Metabolizer® is the only product that we know of in the market, which combines beta sitosterol, beta glucan, soy isoflavones and Chromax® (chromium picolinate) together in one cholesterol support formula.
- Cholesterol Metabolizer® offers this guarantee: If you are not satisfied that after a sixty day trial, it did not support healthier cholesterol levels, we will refund your entire purchase price (less the cost of shipping).
- This Guarantee DOES NOT APPLY to any person who has recently gotten off any statin drug . . . as they will more than likely see an ELEVATION of their levels for a 6 month period.
Cholesterol Metabolizer®: contains four supportive ingredients at a fraction of what they would cost separately
|
Serving Size: 1 Capsule
Servings per container: 60 |
||
| Amount Per Serving | % Daily Value | |
|---|---|---|
| Beta Sitolsterol Complex | 300 mg | * |
|
Beta1,3 Glucan (as Polysaccharide from Avena Sativa) |
120 mg | * |
|
Soy Isosflavones (standardized to contain 40% Isoflavones) |
50 mg | * |
|
Chromium Picolinate (as Chromax®) |
100 mcg | 83% |
Other ingredients: Rice Flour, 100% Vegetable capsule, L-Leucine, Syloid® and water
Directions
Take one capsule in the morning and one in the evening.
Beta Sitosterol
Beta-Sitosterol is a natural plant oil extracted from soybeans, sugar cane and rice. When taken as a dietary supplement, it helps support healthy cholesterol
If there was only one supplement you could take to support healthy cholesterol it would probably be beta-sitosterol. It is, after all, THE most studied healthy cholesterol supporting supplement on the face of the planet. Published medical journal studies actually go back 50 years, yet most people have never even heard of it.
Beta-sitosterol is a phytosterol or plant alcohol that is literally in every vegetable we eat. We already eat this every day but we just don't get enough of it. The typical American is estimated to eat only 200-400 mg a day while vegetarians probably eat about twice this much. Actually the term "beta-sitosterol" in commerce refers to the natural combination of beta-sitosterol, stigmasterol, campesterol and brassicasterol as this is how they are made by nature in plants. There are no magic foods with high levels of phytosterols, but they can be inexpensively extracted from sugar cane pulp, soybeans and pine oil.
Upjohn Pharmaceuticals tried to make a prescription analog (chemical relative) of it decades ago for lowering cholesterol but did not succeed - the natural molecule works best. The scientific community has been well aware of it and clinics around the world have done extensive studies on both humans and animals including gall bladder, bile and liver functions since these are all part of the cholesterol metabolism. The major mechanism this seems to be effective is simply by preventing the dietary cholesterol from being absorbed in the intestines where fat is digested. Another way this seems to work is by increasing the flow of bile acids, which binds the cholesterol in the digestive track and excretes it in the feces.
The research is so extensive and wide ranging over the last 30 years that it is hard to find and count all the studies. How something so studied, and well known to the scientific and medical community has stayed outside of public knowledge is hard to believe.
Beta Glucan

Beta glucan is a polysaccharide found in oats, barley, yeast and mushrooms. For more than 2 decades, medical researchers have been studying the ways by which Beta glucan helps support healthy cholesterol, yet most people have never even heard of it. Most vitamin companies and health food stores don't even sell it.
Beta glucan is a polysaccharide found in oats, barley, yeast and mushrooms and has been used to support healthy cholesterol and healthy immune system responses for more than 2 decades. Beta glucan used to be very expensive to extract but technology has advanced to the point where it can now be extracted very inexpensively.
At the University of Hamburg in Germany it was shown that all 1,3 configuration beta glucans have the same biological potency whether they are derived from oats or yeast -the two major sources
It is interesting that oat and barley have 1,3/1,4 structural arrangements, while yeast and mushrooms are 1,3/1,6 arrangements, regardless, they are all basically true 1,3 beta glucans.
Aside from being an excellent support for healthy cholesterol, beta glucan is also known as an incredible supporter of a healthy immunity response.
Soy Isoflavones
Isoflavones are found in soybeans, chick peas and other legumes. Soybeans, however have the highest concentration of these powerful compounds. Soy contains many individual isoflavones, but genistein and daidzein are the ones which support healthy cholesterol the most.
Isoflavones are an excellent source of support for healthy cholesterol. They are a class of phytochemical compound found only in plants; and are a type of phytoestrogen, or plant hormone, that resembles human estrogen in chemical structure.
Isoflavones are found in soybeans, chick peas and other legumes. Soybeans however, have the highest concentration and also contain many individual isoflavones of which genistein and daidzein are the most supportive.
Dr. Erdman from The American Heart Nutrition Committee (Circulation, December 2000) advised Americans with high cholesterol to add soy protein to their diets.
Chromium Picolinate

Chromium is a very important trace element which is often deficient in our refined diets. Chromium Picolinate is thought to be the best source of chromium.
CHROMAX® is the patented and most effective form of chromium picolinate. It has been tested for two decades and found to be safe and supportive of healthy cholesterol.
The role chromium picolinate may play in supporting healthy cholesterol has been studied extensively. In one study published by "The Western Journal of Medicine" and titled "The effect of chromium picolinate on serum cholesterol and apolipoprotein fractions in human subjects", research suggested that chromium picolinate may support healthy cholesterol.
How Does Cholesterol Metabolizer® Compare To Other Healthy Cholesterol Support Formulas?
There are other healthy cholesterol support products on the market. You are probably interested to know how they compare to Cholesterol Metabolizer®.
Cholesterol Metabolizer® comes in a 100% vegetable capsule. How many (if any) other cholesterol formulas can say that?
Most do not have the same vital endogenous (naturally occurring in the body) ingredients that Cholesterol Metabolizer® contains. Some formulas contain exogenous ingredients (NOT naturally occurring in the body) such as Guggu and Policosanol. Though exogenous ingredients such as these may be supportive, exogenous supplements in general will only support for about six months. Beyond that you will not get any additional support from continuing to use them.
Why continue to take (and pay) for exogenous ingredients in your healthy cholesterol support formula?
There are some cholesterol reducing formulas that DO contain the same endogenous ingredients that Cholesterol Metabolizer® has . . . but take a look at the amount of each ingredient. There is no other product out there that has a whopping 300 mg beta sitosterol, 100 mg beta glucan, 50 mg soy isoflavones and 100 mcg of Chromax® . . . per capsule.
- Both Cholest-Off (formulated by Nature Made) and Cholox (formulated by ProCaps Laboratories) provide beta sitosterol (each with their own proprietary sterol blend), but neither one contains Beta Glucan, Chromax® or Soy Isoflavones. Price: $26.53 (Cholox) $25.95 (Cholest-Off)
- Dr. Derrick DeSilva, M.D. & Unimark Health promote a formula on TV called Cholestium.
- It too DOES contain Beta Sitosterol, but has NO Beta Glucan, Chromax®or Soy Isoflavones.
- And it DOES contain Guggu, which is a fine supplement but . . . being EXOGENOUS has only short time effects. Price: $19.99
- CholesterClear
- WeKnowCholesterol.com- is a site which pretends to be an impartial product review site. In actuality, they bad mouth all products except for one (CholesterClear) and they do not link to any other sites except for that one. That is not exactly impartial. In fact it is just a trick to promote "CholesterClear". Enough about their trick . . . let's look at their product - "CholesterClear".
- They claim that CholesterClear. is better than "Choelsterol Metabolizer®" because it provides 1200 mg of Beta sitosterol. The point they neglect to mention is that there are no studies what so ever which even suggest that taking 1200 mg/day of beta sitosterol provides any benefit compared to taking 600mg/day. CholesterClear is in fact NOT any better than Cholesterol Metabolizer® . . . just more expensive.
- The "CholesterClear" website which WeKnowCholesterol.com describes as being "so informative" does not even list the The "CholesterClear" ingredients. Probably because it more than likely does not even contain the very important cholesterol reducing supplement beta glucan.
- ProgressiveHealth produces a cholesterol reducing formula called Retorol.
- It contains NO Beta Sitosterol what so ever. It does have Vitamin B3, which some people are allergic to and it also contains Guggu which only has short term effects.
- Price: $19.95
- Healthy Choice Nutritionals- produces Cholesterol Care.
- It DOES contain Beta Sitosterol but only1/2 the amount contained in Cholesterol Metabolizer®.
- It DOES contain Beta Glucan but only 1/4 the amount contained in Cholesterol Metabolizer®.
- Price: $27.00
Look at any other cholesterol reducing products out there and ask yourself:
Are the ingredients endogenous? or exogenous?
How much of each endogenous ingredient is there per capsule?
How many capsules does each bottle contain?
What is the cost per bottle?
What is the cost per equivalent dosage?
Once you have done the math . . .
you will know that there is no other product that comes close in offering the amount of healthy cholesterol support per cost . . . as does Cholesterol Metabolizer®.
We Guarantee it !!
Cholesterol Metabolizer® offers this guarantee:
If you are not satisfied after a sixty day trial,that
Cholesterol Metabolizer® supported healthy cholesterol,
we will refund your entire purchase price (less the cost of shipping).
This Guarantee DOES NOT APPLY to any person who has recently gotten off any statin drug . . .
as they will more than likely see an ELEVATION of their levels for a 6 month period.
Cholesterol Metabolizer®
- Promotes Healthy Cholesterol
- Promotes Healthy Immune Response
Contains:
60 capsules per bottle
- Beta Sitosterol
- Beta Glucan
- Cromax®
- Soy Isoflavones
Suggested use:
1 capsule twice per day
- 1 bottle
- $24.95
- 2 bottles $23.95 each
- $47.90
- 3 bottles $22.95 each
- $68.85
- 6 bottles $21.95 each
- $131.70
- 12 bottles $19.95 each
- $239.40
Cholesterol Metabolizer® Supplement Facts
|
Serving Size: 1 Capsule
Capsules per container: 60 Servings per container: 60 |
||
| Amount per Serving | % Daily Value | |
|---|---|---|
| Beta Sitosterol Complex | 300 mg | * |
|
Beta 1,3 Glucan (as Polysaccharide from Avena sativa) |
120 mg | * |
|
Soy Isoflavones (Standardized to contain 40% Isoflavones) |
50 mg | * |
|
Chromium Picolinate (as Chromax®) |
100 mcg | 83% |

*Daily value not established.
Other ingredients: Rice Flour, Vegetarian Capsule, L-Leucine, Syloid® and Water
Directions:
Take one capsule in the morning and one in the evening (preferably with a meal).
Pectin Plus®
Pectin Plus® is the perfect companion product to Cholesterol Metabolizer®
- Supports Healthy Detoxification
- Supports Healthy Cholesterol
- Supports Cardiovascular Health
- Promotes Healthy Blood Pressure
- Promotes Healthy Cell Growth
- Promotes Healthy Immune Response
Contains:
180 capsules per bottle (30 day supply)
- Citrus Pectin
- Garlic Extract (odorless)
- Cilantro Extract
Suggested use:
3 capsules twice per day
- 1 bottle
- $29.95
- 2 bottles $28.95 each
- $57.90
- 3 bottles $27.95 each
- $83.85
- 6 bottles $26.95 each
- $161.70
- 12 bottles $24.95 each
- $299.40
Pectin Plus® Supplement Facts
|
Serving Size: 3 Capsules
Capsules per container: 180 Servings per container: 60 |
||
| Amount per Serving | % Daily Value | |
|---|---|---|
Citrus Pectin
|
1,500 mg | * |
Garlic Extract (oderless)
|
300 mg | * |
Cilantro Extract (20:1)
|
75 mg | * |

*Daily value not established.
Other ingredients: 100% Vegetable capsule, L-Leucine, Syloid®, Rice Flour and Water
Directions:
Take three capsule in the morning and three in the evening.

Other Products available from: NHS Global Distributors LLC



Prostate Miracle®Advanced Formula
2nd generation upgrade to our original Prostate Miracle®. This highly effective, natural, time-tested formula contains pine derived beta sitosterol (NON GMO and NOT Chinese).
read more
LipoProstate Miracle™
3rd generation upgrade to - Prostate Miracle®, using our Advanced Liposomal Delivery System™ to overcome the absorption barriers that men with prostate and gut issues face.
read more
Sea of Greens®
A Whole-Superfood supplement, combining an optimal blend of sea vegetables and Freshwater algae.
read more
Estrogen Balance®
A natural formula for Men & Women, combining: D.I.M., Quercetin and Flaxseed.
read more

Pectin Plus®
Supports healthy detoxification, healthy blood pressure, healthy cholesterol levels and prostate health
read moreContact
255 Rivertown Shops Dr.
Suite 102, PMB 128
Saint Johns, FL 32259
International: 1.805.322.0005

Thank you for visiting Cholesterol-Metabolizer.com
This information here within is designed to provide accurate information in regard to the subject matter covered. It is provided with the understanding that NHS Global Distributors LLC is not engaged in rendering medical advice. If expert assistance is required, the services of a competent medical professional should be sought. These statements have not been evaluated by the Food and Drug Administration. These products are not intended to diagnose, treat, cure or prevent any disease. Always read and follow manufacturer's directions that come with this product.
You are protected by the FDA Dietary Supplement and Nonprescription Drug Consumer Protection Act
please call 877.965.2140 or Click here to report any Adverse Reaction with Cholesterol Metabolizer®